Axios Future of Health Care

April 26, 2024
1 big thing: Hospitals' forced makeover
Illustration: Gabriella Turrisi/Axios
2. The emerging divide
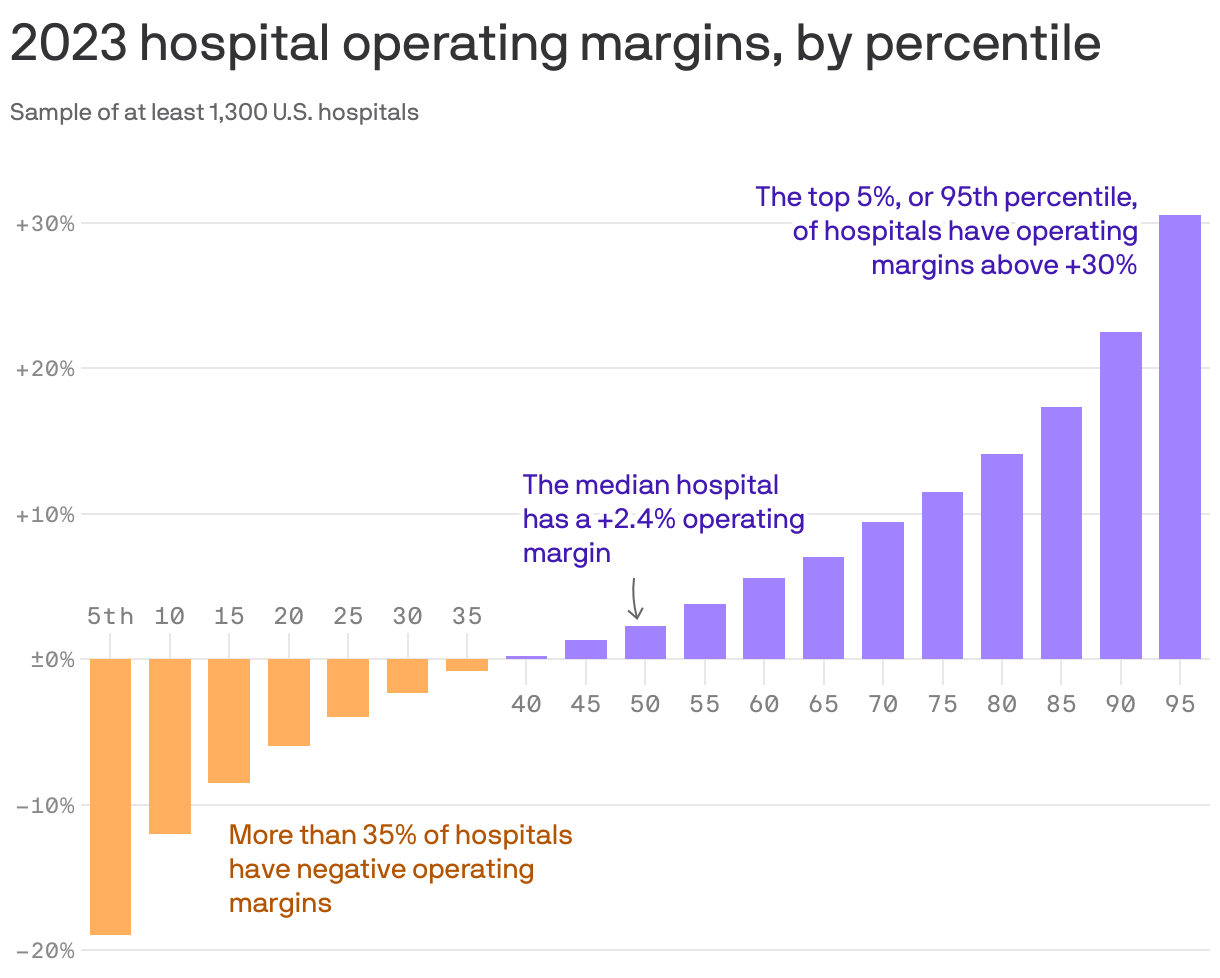
Some health systems have recovered from the pandemic much better than others, and those with healthier margins tend to be the ones that made a stronger push into outpatient care.
By the numbers: There's a wildly large and growing difference between the operating margins of top-performing health systems and those at the bottom, according to Kaufman Hall data shared with Axios. (Go deeper on their analysis.)
- "The hospitals that are not performing well are performing worse, but the hospitals that are recovering are performing extremely well," firm co-founder Kaufman told Axios.
- "I would say hospitals that are not doing particularly well … they're not capturing that outpatient work, or at least not at the level that they need to," he added.
Yes, but: Operating margin is only one measure of a hospital's financial health, and total margins are often much higher, said Anderson, the Johns Hopkins professor.
- "You diversify where there is potential profit, and they have moved into all sorts of things where there is profit," he added. "They have a whole portfolio of ways to make money now that they didn't have 20 years [ago]."
- Some experts also say that hospitals aren't disciplined about keeping costs down.
- "I think partly what happened over time is that … investments were not treated as investments, but as costs," said Cooper, the Yale economist.
3. The hospital of the future

Illustration: Sarah Grillo/Axios
Axios Future of Health Care

Keep up with health care politics, policy and business