Axios Future of Health Care

August 30, 2024

1 big thing: Into the hospital margin rabbit hole

2. Diving into the weeds
Time to get wonky about margins! Let's start with the topline:
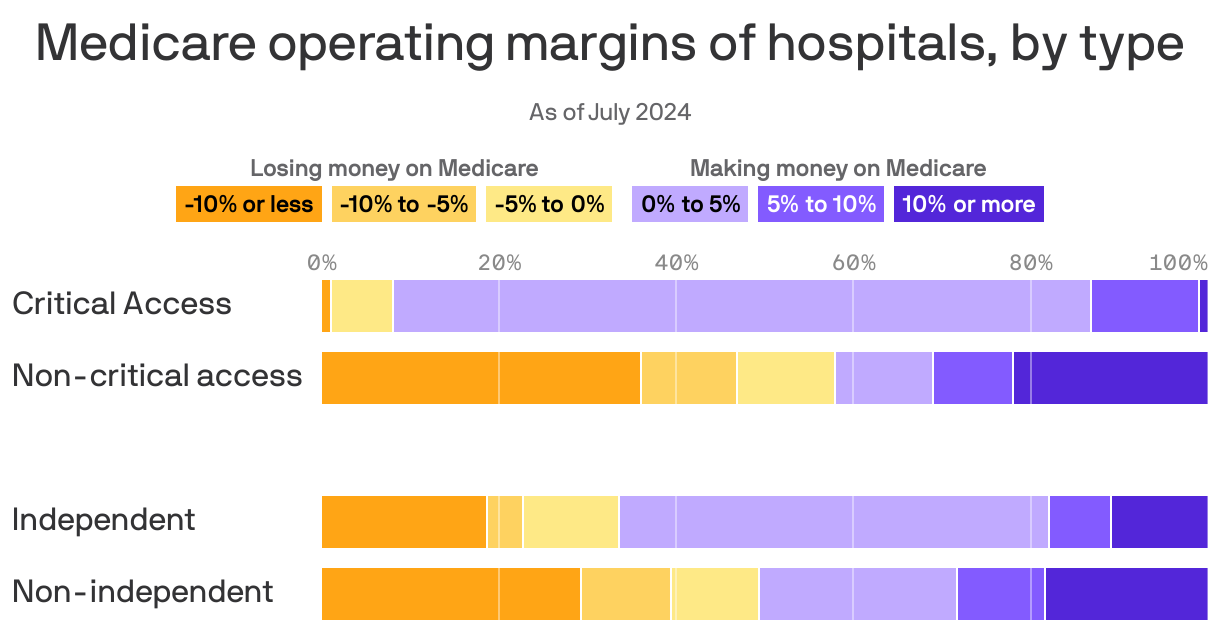
- The Third Way analysis found that 55% of hospitals made money on Medicare in 2022, based on hospitals' own financial reports.
- Third Way combined traditional Medicare and Medicare Advantage for this analysis. The data they used show that Medicare margins are, on average, -5% for traditional Medicare and 0% for Medicare Advantage, author David Kendall told me.
- MedPAC, on the other hand, reported earlier this year that hospitals' average Medicare margin fell to a "record low" in 2022, which was -11.6% (This is the number quoted by the AHA if you recall from above).
Details: Third Way used a dataset compiled by the National Association for State Health Policy and supported by Arnold Ventures that uses cost reports submitted by hospitals to the federal government.
- The AHA in its blog post argued that the dataset "inflates hospitals' margins by both undercounting hospital costs as well as incorrectly counting hospital revenue (including by assuming revenue that demonstrably does not exist)."
I called up Arnold's Miller to discuss the differences between the datasets since he's a former MedPAC executive director in addition to his current title.
- He said the datasets have different purposes, so neither is the "right" one. But he wanted to talk more about the fake costs idea, and he said Third Way's finding that independent hospitals have better Medicare margins than health systems makes perfect sense.
- "If you have pressure from your revenue, you actually contain your costs. But if you're a large hospital system, you have a consolidated position in the market, you're not under fiscal pressure and your costs are higher," he told me.
- "The richest hospitals in this country have the worst Medicare margins. It's so much revenue that their costs follow the revenue, and that, of course, made them much worse on Medicare."
When you hear hospitals talk about "investments," those are costs. At a very high level, they can be broken down into clinical and non-clinical spending.
- "Imagine I make lots of profits in one year and I decide to build a new cancer center or I choose to recruit a bunch of really good doctors at really high pay. That's going to make my costs pretty high," Yale's Cooper said.
- "I'd rather them go to high-quality doctors than self-playing musical instruments in the lobby," he added.
The bottom line: Separate research has found that hospitals with more potentially privately insured patients have higher quality, which takes money.
- "As the spread between private and Medicare goes up, you're more incented to attract more privately insured patients, and part of the way you attract more privately insured patients is really investing in things that privately insured patients want," Cooper said.
My thought bubble: Thanks for coming with me on this journey, where we basically ended up at the idea that hospitals' costs may be related to the kind of patients they want to — or do — attract. And that's not people with lower-paying government insurance, at least when looking at it through a financial lens.
- That seems to me like a pretty big idea in itself — hit reply if you have thoughts!
3. Axios Interviews: Focusing on quality

Axios Future of Health Care
