Axios Future of Health Care

July 26, 2024

Good morning. Today we're going to talk a little more than usual about politics — but not those politics. You know, the stuff that's been consuming our lives for the last two weeks or so.
Today's word count is 1,551, or a 6-minute read.
1 big thing: What Washington's anti-consolidation push misses

Attacking consolidation and related anti-competitive business practices in health care has emerged as something of a bipartisan cause over the last few years. There's just one big problem: Health care already is heavily consolidated, and most of the solutions can't change that.
Why it matters: Whether it's insurers, pharmacy benefit managers, hospitals or providers, today's health care landscape is increasingly dominated by large players wielding outsize market power, which experts say contributes to high and rising costs.
- Most policymakers worried about health costs are still generally united around approaches that use market forces to lower or at least stabilize prices. Many measures that would ultimately help prevent future consolidation and preserve competition have widespread appeal.
- But a question that often goes unaddressed is, what to do about markets where there's little to no competition?
- "The term that is used when you talk about trying to unwind consolidation that's already happened ... is unscrambling the eggs," said Leemore Dafny, an economist and Harvard Business School professor. "That's so exceedingly difficult that their energies are focused on prevention."
The answer, experts say, has to be some combination of government cracking down on anti-competitive business practices, regulating prices, or directly or indirectly breaking up big companies.
- Spoiler: I can't find anyone advocating for the FTC or the DOJ to swoop in and start engaging in early 20th century-style trustbusting, although some ideas could have the effect of breaking up large companies.
- And while there's decent support for measures like price transparency or prohibiting anti-competitive contracting, those alone probably won't undo the downstream effects of consolidated markets.
- That leaves government price regulation — an approach supported by even some staunch free-market advocates. But aside from prescription drug prices, it's an option even progressive Democrats shy away from when dealing with the commercial sector.
- "It is hard to look ahead and see that we are going to correct, in many settings, the lack of competition that we observe," Dafny said. "And so if we don't have competition, unless you want unfettered monopoly power, you need some kind of regulation."
Catch up quick: PBMs have had a particularly newsy month and were the subject of both a House Oversight Committee report and an interim FTC report.
- Both point out how the largest three PBMs control about 80% of the market and are vertically integrated entities that also own insurers and pharmacies.
- Insurers also increasingly own providers (read Stat's excellent investigation on how UnitedHealth "exploited its growing power to milk the system for profit," which was co-authored by my old pal and former Axios colleague Bob Herman).
- Vertical integration has its virtues; economists can see how an integrated payer model would lead to cost savings, for example.
- "Conceptually, there's a lot to like about it, but that only works downstream to benefit patients and payers if there's competition," Dafny said.
Zoom in: Despite the recent attention on the payer side, the first place most of the experts I spoke with gravitated to was hospital consolidation.
- That's also where Congress has focused most of its attention over the past couple of years.
- That's at least partially because there's better research on the impact of hospital mergers and provider acquisitions than other forms of vertical integration, and research has found over and over that concentrated hospital markets lead to higher prices.
- But it's also the segment of the medical system where the question of what to do about concentrated markets is most relevant and, given all of the attention it's received, the obvious elephant in the room.
- "A major challenge of antitrust policy is that many provider markets are already highly concentrated, and it's difficult to break up mergers or unwind mergers after they've already occurred," said KFF's Zach Levinson.
The other side: Hospitals say mergers and acquisitions enable them to expand patient access, keep financially struggling facilities afloat and have a strong footing in negotiations with large national insurers.
Let's go deeper below...
2. The solutions

Let's start by talking about the bucket of policies that Congress or the Biden administration are pursuing.
- Particularly in the House, there's been bipartisan interest in measures promoting hospital price transparency and aligning payment rates for different settings of care, known as site-neutral payments. There's also been chatter (mostly among Democrats) about increasing resources and authorities for the FTC to pursue antitrust cases.
- The FTC has been aggressive in challenging health care mergers under President Biden, and the administration this year put out a request for information about consolidation in health care markets.
- But "I do think there is a lot of consolidation in the rearview mirror, and unless the FTC is really talking about breaking up some of these big systems — which I'm not hearing — I do think it's mostly preventative," said Mark Miller, executive vice president at Arnold Ventures.
- Banning what experts say are anti-competitive practices among providers, or those that generally lead to higher health care costs, could both curb the downstream impact of consolidation and remove the incentive for future combinations, by making them less lucrative.
- "What you're trying to do is take the juice out of consolidation," Miller said.
Yes, but: At the think tank level, things get a little more interesting — there's way more talk about price regulations.
- Experts still have differences over the extent to which market competition is itself a solution. But there's pretty widespread buy-in to the idea that the government will have to do something to fix broken health care markets.
- Proposals by the Bipartisan Policy Center, the Hamilton Project (which Harvard's Dafny coauthored), the Foundation for Research on Equal Opportunity and the Progressive Policy Institute include some kind of price cap.
The intrigue: This section is light on payer-side solutions because most people don't seem to know what to do, or say that being big isn't the root cause of insurers' or PBM's anti-competitive practices.
- "It's not just United. United is just the best at all of this," Miller said. "If there are limitations on how much money they can make — if they get consolidated but they can't engage in the upcoding — maybe I'm less concerned about it."
- And some experts say payer consolidation is at least in part a response to provider consolidation.
Others are more concerned about the mere existence of such large companies. (One of the ironies about the way the Change Healthcare cyberattack put the spotlight on UnitedHealth Group's size is that the DOJ unsuccessfully challenged the acquisition in 2022.)
- An idea that's been floated by the American Economic Liberties Project — an anti-monopoly think tank — is for Congress to simply ban insurers and providers from being owned by the same company, which would effectively break up a behemoth like UnitedHealth.
The bottom line: "If we're getting serious about policy, this really isn't a question about government intervention or not," said Hayden Rooke-Ley, a senior fellow at AELP who recently wrote a white paper on Medicare Advantage and vertical consolidation.
- "I think we've had these fallacies about these markets being natural and having this bias against governing," he added. "It's left us with a system that's so irrational, so inefficient and so wasteful, and preserves this idea that the government isn't involved when the government is deeply involved in these dynamics."
3. Throwback content
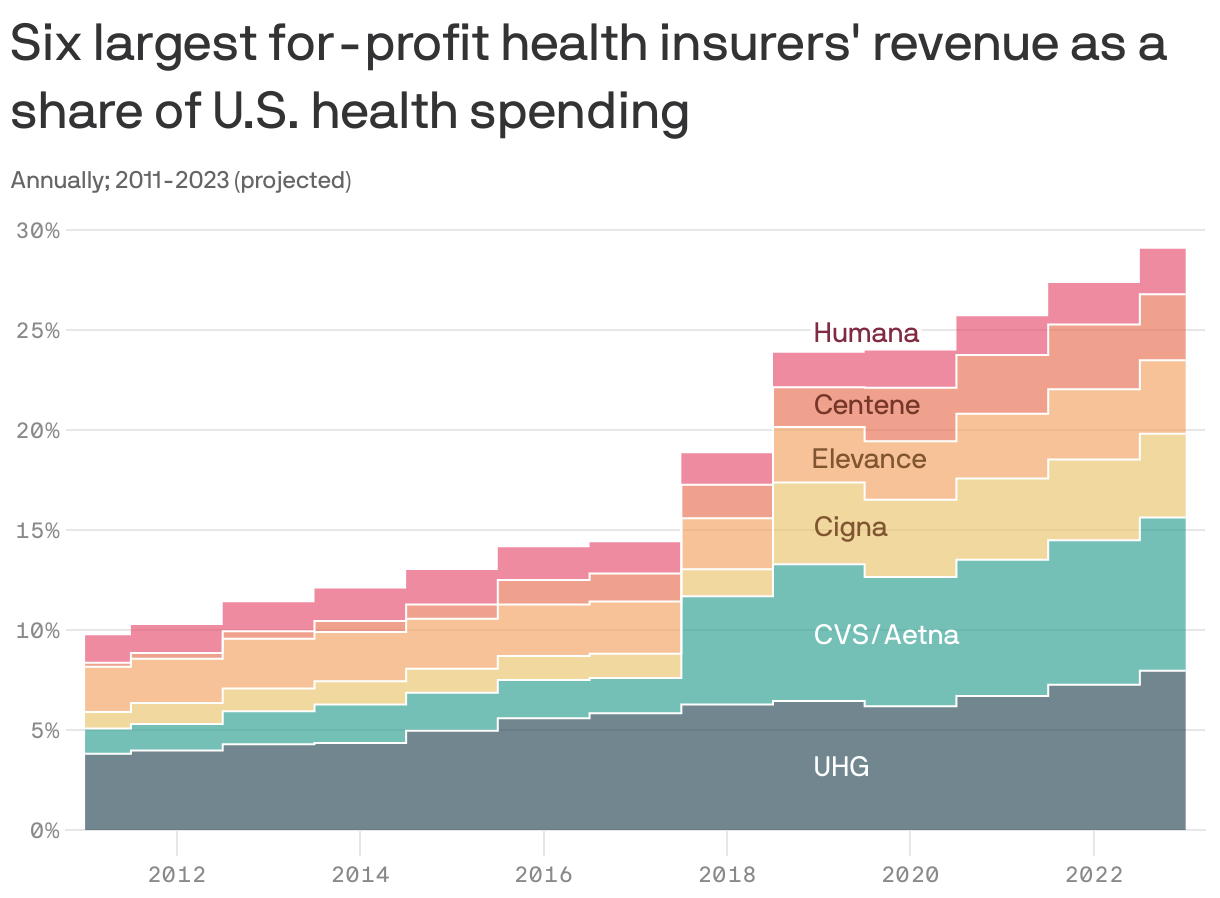
We've been talking about vertical integration for a while now — remember this chart?
If you want a refresher on big insurance-plus companies, here's the link to one of our very first Future of Health Care newsletters.
4. The free market case for price caps
I want to go deeper on one think tank plan in particular, partially because it's been turned into actual legislation on the Hill — and also because both versions are coming from the political right.
How it works: The plan, originally developed by the Foundation for Research on Equal Opportunity, would cap payment rates for commercial payers at Medicare Advantage rates in "extremely concentrated hospital markets," with exemptions for rural hospitals.
- If hospitals in those markets didn't want to get paid MA rates — which generally are much lower than commercial rates — they could opt to break up instead.
- Rep. Jim Banks, who is now running for the Senate in Indiana (and whom no one would accuse of being too liberal), has a bill that incorporates this framework.
Between the lines: "The foundation of the idea is that the FTC is not inclined…to go after mergers that have already taken place and forcibly break up health systems. They're very worried about the disruption that would cause to health care," FREOPP president Avik Roy told me.
- His plan "is kind of like auto antitrust, because basically the hospital system will decide," he added.
- "But if you're going to be concentrated, then we have to create some sort of countervailing force to make sure that you're not exploiting your monopoly power."
I was curious how many hospital markets the Banks bill would apply to, so I did some very back-of-the-envelope math.
- Using the concentration threshold outlined in the legislation, I used this 2021 dataset from the the Health Care Cost Institute to see how many metro areas met that threshold.
- The answer: 51 of the 183 areas, or nearly 28%.
The bottom line: This is a really interesting example in which government intervention is seen as allowing market forces to work, not standing in the way of them.
Thanks to Nicholas Johnston and Adriel Bettelheim for editing and Cindy Orosco-Wright for copy editing.