Axios Future of Health Care

June 21, 2024

Good morning. I'm back from a very restful vacation, although admittedly I am still catching up on your emails.
- This is the last edition of the inaugural deep dive newsletters! Hit reply if you want to help me figure out what to write about next week.
Today's word count is 1,008, or a 4-minute read.
1 big thing: Inequality's long reach

We've spent the last nine weeks going through health care's defining topics, but if there's a thread tying them all together it's this: Health care in America is deeply unequal, and it might get worse.
Why it matters: All of the innovation in the world won't make any difference to patients if it's unaffordable or inaccessible, and right now everything in the pipeline is headed for a two-tiered system.
- "It's not only inequities in access to the system, but then also differential experiences even within the system," said Samantha Artiga, vice president and director of the Racial Equity and Health Policy Program at KFF.
- When you look at health outcomes, "you will see persistent and long-standing disparities in health … really from the beginning of life to end of life."
While some groups of Americans are undoubtedly better off on the whole than others, there can be substantial variation even within socioeconomic groups.
- "People have multiple identities and don't fit into one single box, so their experiences are going to be shaped by who they are based on multiple different dimensions," Artiga said.
Where it stands: Disparities are a key part of every conversation we've had so far. Here's how:
- Insurance: Most people of color are less likely than white people to have insurance, and people who are uninsured face much higher barriers to care than those with insurance.
- Among those with private insurance, low-income enrollees pay a much larger share of their overall budget toward health care than higher-income enrollees, primarily on premiums, according to a recent JAMA Internal Medicine study.
- And, of course, not all insurance is created equal. The insurance you have is determined largely by your income, employment or age, and plans can have strikingly different out-of-pocket requirements and coverage networks.
2. Hospitals: Insurance disparities also directly tie into hospital care, since a facility's financial health is connected to the types of patients it serves.
- Hospitals with larger Medicare, Medicaid and uninsured populations have limited ability to draw in more revenue through privately insured patients. These hospitals are often the ones closing completely or cutting service lines — or are at least less likely to be building new state-of-the-art facilities.
- Hospitals tend to be racially segregated, a reflection of ongoing residential segregation, and a recent study found that higher segregation of hospital care was associated with worse health outcomes for Black and white Medicare beneficiaries.
3. Prescription drugs: This one's pretty obvious — you hear all the time about patients forgoing medication because they simply can't afford it.
- Racial disparities trace back to the very beginning of the development process, as people of color are underrepresented in clinical trials.
- As multimillion-dollar drugs continue to hit the market, access will be dependent on type of coverage. State Medicaid programs and small businesses that provide health insurance will have the toughest time affording these advances.
- And the new class of anti-obesity drugs are potentially foreshadowing a future in which some medical products or services are significantly more available to people who can pay for them out of pocket, circumventing insurance barriers.
4. Access: Most people of color are more likely than white people to not have a doctor or to have gone without care due to cost, per KFF.
- People who live in rural areas may not physically have access to doctors or even hospitals near where they live.
5. Aging: Lower-income seniors are more likely to have disabilities and die younger.
- Even though age is the sole criteria for Medicare coverage — which is highly regulated — a larger share of Black and Hispanic beneficiaries report trouble getting care than white beneficiaries.
2. Inequities, continued

6. Mental health: Among adults with a mental illness, white people are significantly more likely to receive treatment than Black, Hispanic or Asian people.
- Access to mental health treatment is notoriously difficult, but it's even harder for people who can't pay out of pocket for care, because they can't find a provider who takes their — or any — insurance.
7. Addiction: The opioid epidemic began as a phenomenon primarily among rural white Americans but has morphed into a polysubstance crisis, and the highest overdose death rates are now among American Indian and Alaska Native and Black Americans.
- There's also the criminalization element: Although racial and ethnic groups use substances at similar rates, Black Americans face a disproportionate rate of drug arrests.
8. Workforce: Many of today's access issues are at least partially a result of workforce shortages, which create a scarcity of care.
- It's within this context of scarcity that certain people — either by virtue of their income or insurance type — have better access to care than others, and those with the resources to do so can bypass the line altogether through concierge care.
- Some experts have raised concerns that workforce shortages will ultimately lead to an even more pronounced two-tier health care system. For instance, one worry is that the best doctors will be drawn to well-paying concierge practices, leaving patients who can't afford it with lesser care, AARP writes.
9. Emerging technology: It's not hard to imagine how advances in precision medicine, gene editing or medical forecasting could end up primarily benefiting the select few who can afford them, particularly if policymakers don't come up with a good way for the system to absorb their costs.
- And experts warn that AI algorithms could bake in existing biases or inequities.
3. The bottom line
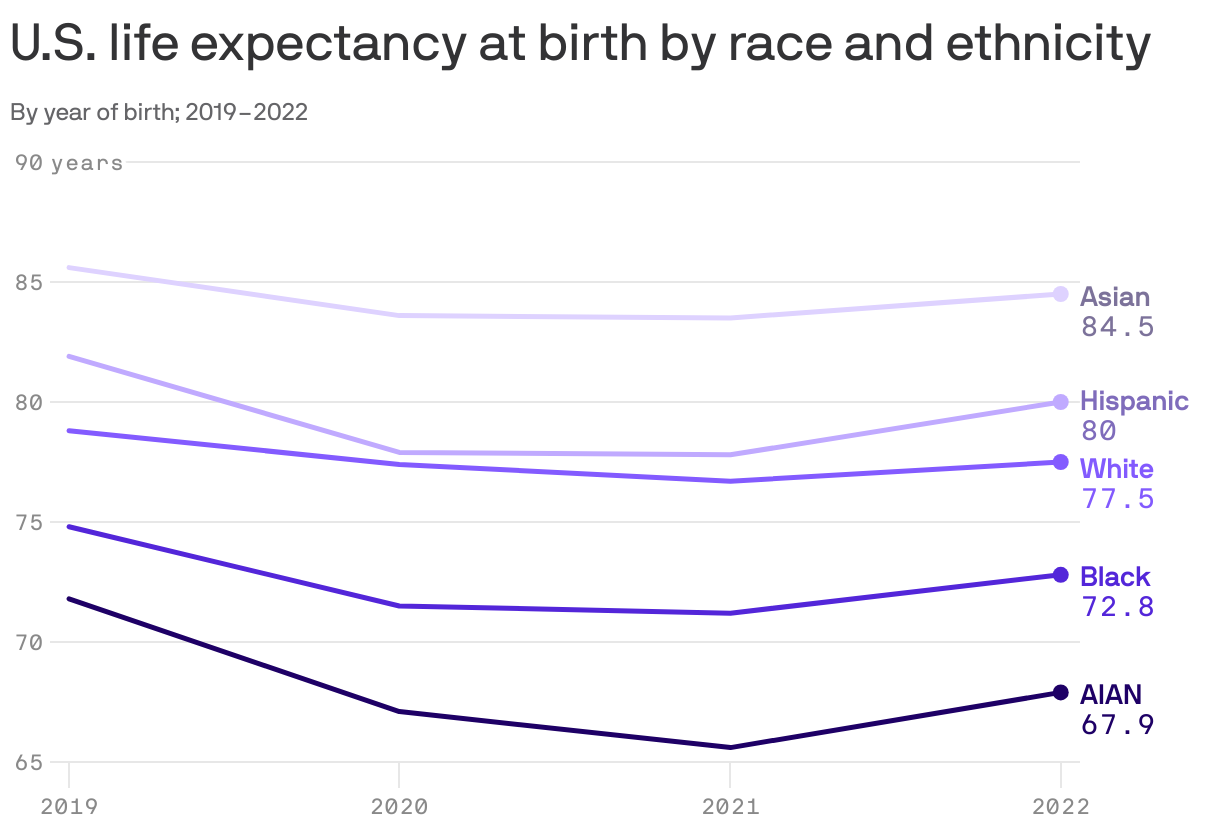
All of these disparities ultimately show up in one very concrete measure: life expectancy, which varies by race, income, education and even occupation.
The big picture: We can talk all day about disparities in access to the health care system and inequities in experiences within that system.
- But a person's health is determined by nearly every facet of their life.
- "People's health is shaped by so many factors that sit outside the health care system and play such a large role," including where they live, their access to nutritious food, their access to transportation and their employment, KFF's Artiga said.
- "All those factors are influenced by underlying structural inequities."
Rereading some of the stories from the last couple of months made me realize that so far, this newsletter has been kind of grim. That's OK, health care can be pretty grim!
- Going forward, we'll try to talk more about solutions. That said, this newsletter isn't about hype — I won't waste your time with that.
- But there's also a lot of cool stuff out there and a lot of ideas about how to solve some of these huge issues. Tell me about some of them!
Thanks to Nicholas Johnston and Jason Millman for editing and Matt Piper for copy editing.
Sign up for Axios Future of Health Care
