Axios Vitals

November 03, 2025




2. Top drug regulator resigns, claims retaliation
George Tidmarsh, the FDA's top drug regulator, abruptly resigned yesterday after federal officials began reviewing "serious concerns about his personal conduct," AP reports.
- In an interview with The New York Times, Tidmarsh claimed a "toxic environment" at the FDA and said the review was retaliation for warnings about politics trumping science in the drug review program.
Tidmarsh's ouster is the latest in a string of leadership changes at the agency, which has been rocked for months by firings, departures and controversial decisions on vaccines, fluoride and other products.
- Tidmarsh, an M.D., was director of the Center for Drug Evaluation and Research, the FDA's largest division, which has lost 1,000+ staffers over the past year to layoffs or resignations.
Tidmarsh was placed on leave Friday, HHS press secretary Emily Hilliard said. Tidmarsh then resigned yesterday.
- A drugmaker connected to one of Tidmarsh's former business associates, Aurinia Pharmaceuticals, said in a lawsuit that Tidmarsh used his FDA position to pursue a "longstanding personal vendetta" against a company executive.
Tidmarsh founded and led a series of pharmaceutical companies over several decades in California's pharmaceutical and biotech industries.

5. Charted: Menopause legislation by state

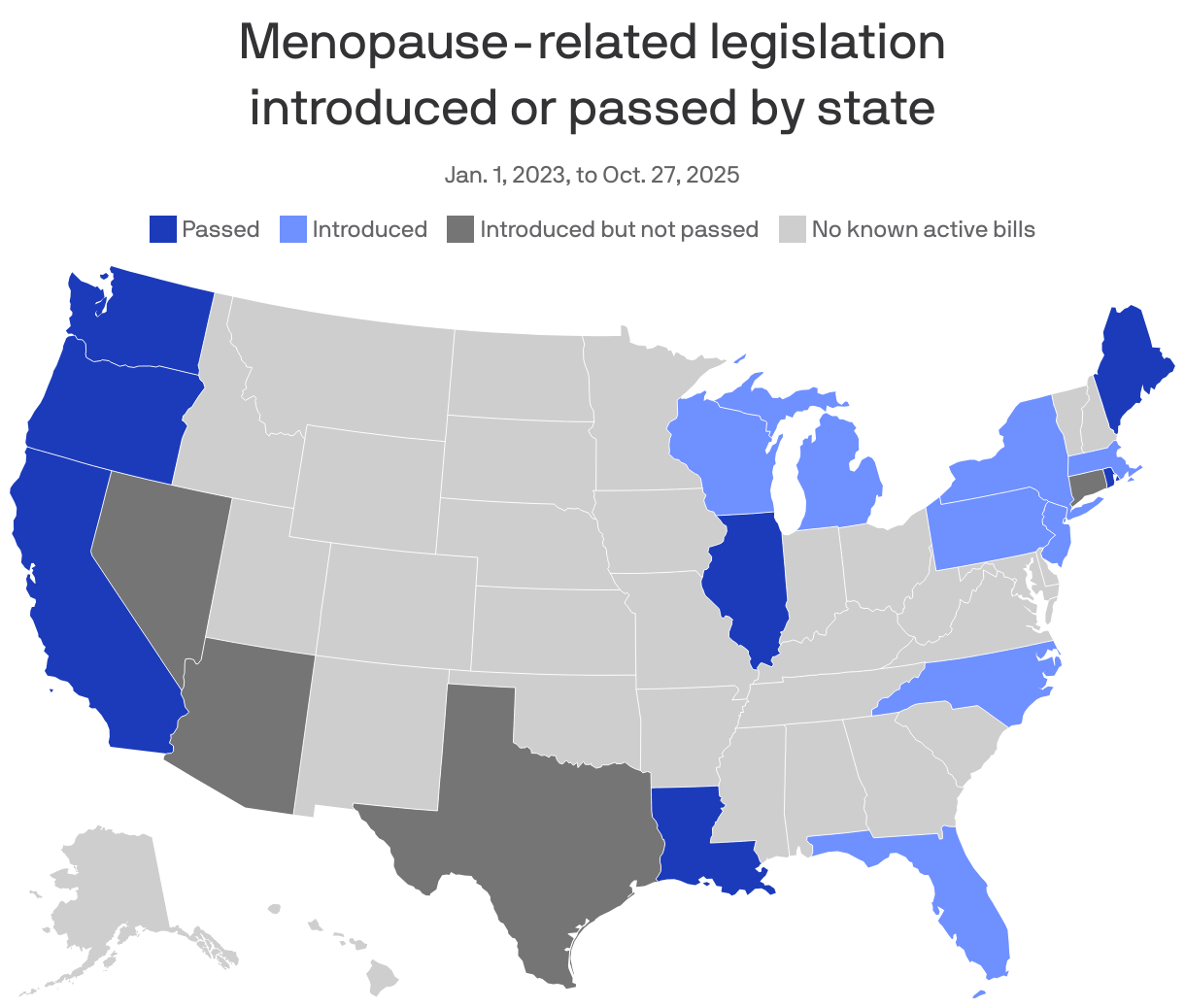
Seven states have passed legislation aimed at promoting menopause care, and at least 36 bills have been introduced in 18 states in a sign of how the condition is becoming more of a policy and health care priority.
Why it matters: Changes like mandates for insurance coverage of treatments in Louisiana and Illinois could not only make treatments more affordable, but bolster workplace support and increase medical training.
- 2025 is already "a watershed year — and was only just the start. Expect to see even more momentum in 2026," Jennifer Weiss-Wolf, executive director of the Birnbaum Women's Leadership Center, told Axios.
State of play: Millennials, the generation that currently includes the most women in America, are heading into the menopause years.
- Celebrities are launching telehealth companies and saying "women deserve better." Influencers are pushing products, which may or may not have scientific backing.
- Gen X and millennial women also are becoming more vocal about the weight gain, hot flashes, brain fog and other symptoms, posting online about their ordeals and pushing providers for better answers.
6. While you were weekending

Axios Vitals
