Axios Future of Health Care

August 16, 2024

1 big thing: Analysts shrug

2. Why this may not be a good crystal ball
3. Anti-obesity drug coverage price tag
Speaking of Medicare spending — if you are paying any attention at all, you know that there's a huge debate over whether Medicare should cover anti-obesity drugs.
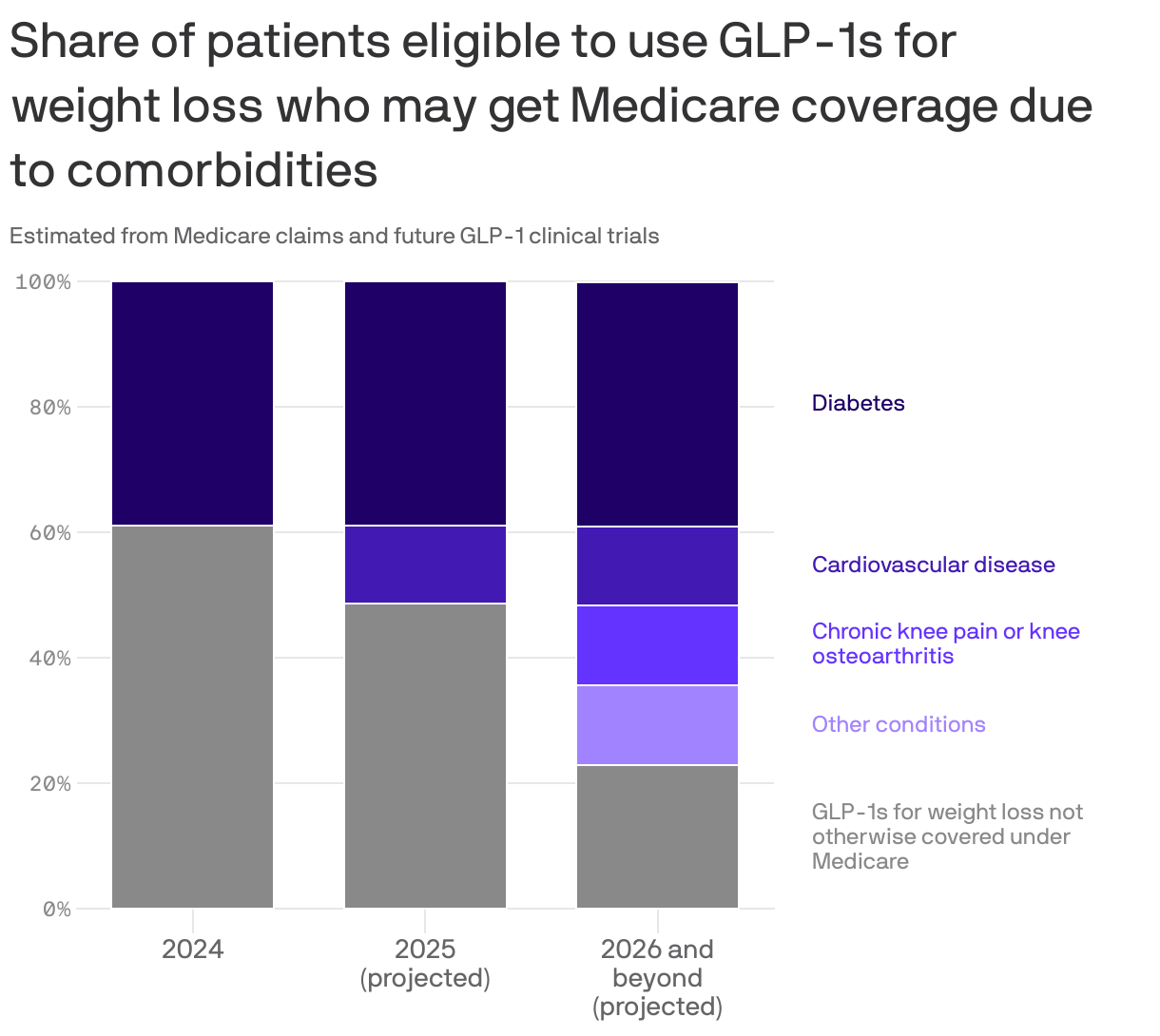
Driving the news: A newly published study in Health Affairs not only gives an estimate for how much such coverage would cost taxpayers, but also illustrates how this may be an overblown debate given all of the other conditions GLP-1s may soon be approved for.
- Medicare already covers them as diabetes treatments, for example. If it also turns out they are effective against knee pain, Medicare would have to cover them for that use in the next few years — it's just weight loss it doesn't cover.
- And millions of patients who'd qualify to use GLP-1s for weight loss have these other conditions that may soon make them eligible for coverage anyway.
By the numbers: The study estimates Medicare coverage, if it started in 2025, to increase spending by $3.1-$6.1. billion a year.
- A very important variable: Those numbers assume only 5%-10% of the newly eligible patient population are prescribed a GLP-1 for weight loss.
The intrigue: Just to go full circle here, semaglutide — the active ingredient in Wegovy and Ozempic — is expected to be eligible for Medicare negotiations as soon as next year, which would mean a 2027 price implementation date.
- That makes estimating how much weight loss coverage would cost even more complicated.
Axios Future of Health Care
